Penny broke into a big grin and said, “I’m so glad you came! Can you get me some coffee?” Sure, I could do that. I also offered to bring her a sack of plain Wendy’s hamburgers, which I knew was one of her favorite meals. She clapped her hands in delight. I gave her the thick wool socks and gloves I had brought along for her, as well as some homemade high energy snacks. I wished I could do more. I offered to take her to a shelter. She explained that she had tried every shelter in town and that her body just couldn’t tolerate the pesticides and cleaners and disinfectants used in them. She had become severely ill from those exposures. I understood that. She was in a really tough situation.
Penny had been a straight A student in High School and had a typical upbringing. She married and had a son. She worked as a waitress at a little cafe on Main Street and was living a happy life until the day the restaurant was sprayed with pesticide. She became violently ill and passed out. Other employees carried her next door to the clinic. She was having great difficulty breathing and almost died. When she finally began to recover, the doctor told her she could not go back to work and would have to avoid further exposure to pesticide.
She had a difficult choice to make. Her family needed the income from her job, yet she was risking her life to go back into that toxic environment. She decided to try working again, but became seriously ill. In time, she lost her job, her family, her home, and her health. No longer able to tolerate any environment that had been sprayed with pesticide, she tried living in first one apartment, then another, but they had all been treated with pesticide. Finally, in desperation, she had begun living outdoors where she could breathe easier.
That is how I met her. People in town just called her “The Bag Lady”, but Mom and I knew she had a story. We used to take her hot meals on cold days. It took a long time before she fully trusted us, but when she finally did, her whole face would light up when she saw us coming. Various agencies tried to help her, but her body would not tolerate indoor environments. One day she shared her story of how she had ended up on the street and showed us a little duffel bag nestled among her other supplies on one of her carts. That bag was stuffed full of articles about allergies, chemical sensitivity, reactive airways disease, and other medical issues. The articles were organized into categories and her filing system would put mine to shame. She spent many of her days in the library and had carefully cut out articles about her illness from magazines that people were giving away. She knew what was wrong. She just didn’t know what to do about it.
Then came the day that we couldn’t find Penny. We had searched around town and even asked the librarian if she knew where Penny had gone. No one knew. By chance (although I know it was really God’s timing) I was driving through downtown Joplin one day and thought I saw Penny’s carts outside the library. I parked and went in. There sat Penny, who was thrilled to see me. She had caught a ride to Joplin, in hopes that they had more resources to help her.
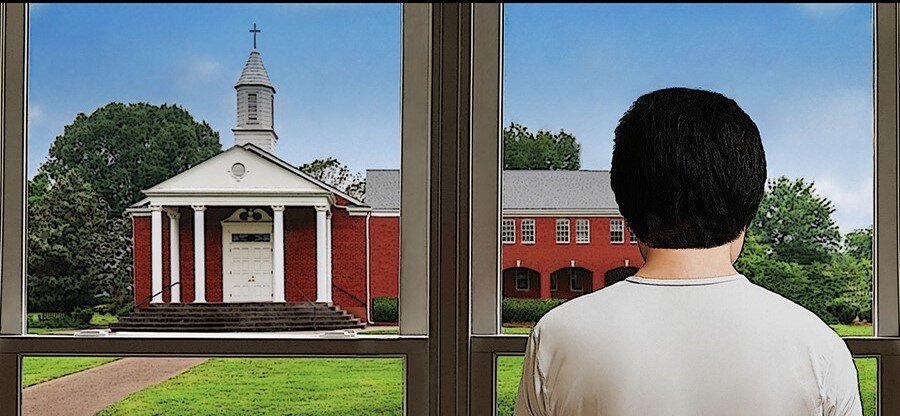
When the library closed, I walked with her back to the spot where she was living. A couple of guys from a church down the street wandered by handing out Bible tracts. While one of them talked to her, I asked the other one if Penny could possibly come into their lobby long enough to warm up on the coldest days. That man looked like I had just asked him to pay off the national debt! Why, NO, she couldn’t come into their church building. Well, not unless she planned to come to church regularly and tithe! I tried to explain why they could not count on her attending church. The man looked very uncomfortable and you could tell he just wanted to be anywhere but standing there talking to someone who was asking him to help a homeless person. I frankly was appalled at his lack of compassion.
It wasn’t long before Mom and Dad went to Joplin for a medical appointment. It was bitterly cold and they had a sleeping bag and warm boots and gloves for Penny. They were disappointed when they couldn’t find her. Suddenly, Mom spotted her carts outside a downtown bar. Now, my mom had never been in a bar in her life, but she marched right in. Penny was seated by a front picture window. She explained that she had gone to the downtown church and asked if she could come in to warm up. They told her NO and turned her away. Meanwhile, the owner of the bar saw her suffering in the cold wind and had gone to invite her in. He told her she was welcome to stay until the bar closed at 2 AM and he brought her a hot meal. I will let you draw your own conclusion about who showed her Christian compassion.
These thoughts were going through my head as I started to go get hamburgers and coffee for Penny on that stormy winter night. A mixture of snow and sleet was coming down and I knew it wouldn’t be long before the roads became hazardous. As I got in my truck she hollered, “Could you get me one more thing?” I said, “Sure” and came back to see what she needed. Well, she asked for cigarettes. I hesitated and said, “I don’t think I can get you cigarettes.” She looked puzzled and said, “You’re over 21, aren’t you? Of course you can buy me cigarettes. You would be surprised how much a lit cigarette can warm up your hands on nights like this.”
Hmmm…. now I had a dilemma. I had never purchased cigarettes and really didn’t want to get them for her. I debated about what to do. Then, somewhere in my spirit, I heard a little voice say, “Who are you to judge her? You are going home to your nice warm house. She is spending the night .. and the next … and the next under a tarp in freezing cold weather. Help her any way you can.” She got her hamburgers and coffee -- and cigarettes.
With this current cold weather, Penny has been on my mind. There are countless people homeless, just trying to survive the day. Perhaps you will have an opportunity to donate your time or money to help them. Perhaps you can say an extra prayer for all those who are homeless. Perhaps God will lead you to meet your own “Penny”. Jesus cared about those people that society ridiculed or forgot. May we all follow His example.
“You will be judged on whether or not you are doing what Christ wants you to. So watch what you do and what you think; for there will be no mercy to those who have shown no mercy. But if you have been merciful, then God’s mercy toward you will win out over his judgment against you. Dear brothers, what’s the use of saying that you have faith and are Christians if you aren’t proving it by helping others? Will that kind of faith save anyone? If you have a friend who is in need of food and clothing, and you say to him, ‘Well, good-bye and God bless you; stay warm and eat hearty.’ and then don’t give him clothes or food, what good does that do?”
James 2:12-16